" height="2.0768733066194303px" id="D9zvikPGQ" transform="translate(2.998 0.199)" width="5.731236321640176px"/><path d="M 0.187 0.574 L 3.457 3.297 C 3.457 3.297 3.662 3.483 3.885 3.483 C 4.089 3.483 4.312 3.297 4.312 3.297 L 7.582 0.574 C 7.713 0.481 7.768 0.313 7.675 0.163 C 7.601 0.014 7.415 -0.042 7.267 0.033 L 4.182 2.103 L 3.903 2.271 C 3.885 2.271 3.847 2.271 3.81 2.271 L 3.531 2.103 L 0.447 0.033 C 0.298 -0.042 0.131 0.033 0.038 0.163 C -0.036 0.313 0.001 0.481 0.131 0.574 Z" fill="rgb(0, 0, 0)" height="3.483465559558452px" id="XHPDa9C06" transform="translate(1.975 1.124)" width="7.7215397232611345px"/><path d="M 1.933 5.727 C 2.063 5.652 2.1 5.503 2.044 5.372 L 0.966 2.91 C 0.966 2.892 0.966 2.873 0.966 2.854 L 2.044 0.392 C 2.1 0.262 2.044 0.113 1.933 0.038 C 1.803 -0.037 1.654 0.001 1.58 0.131 L 0.112 2.519 C 0.112 2.519 0 2.705 0 2.873 C 0 3.078 0.112 3.246 0.112 3.246 L 1.58 5.634 C 1.654 5.745 1.803 5.783 1.933 5.727 Z" fill="rgb(0, 0, 0)" height="5.752520201428617px" id="fSIVTyYyB" transform="translate(9.688 3.208)" width="2.0692037208998664px"/><path d="M 2.899 0.187 L 0.186 3.47 C 0.186 3.47 0 3.675 0 3.899 C 0 4.104 0.186 4.328 0.186 4.328 L 2.899 7.611 C 2.992 7.741 3.159 7.797 3.308 7.704 C 3.456 7.629 3.512 7.443 3.438 7.294 L 1.375 4.197 L 1.208 3.918 C 1.208 3.899 1.208 3.862 1.208 3.824 L 1.375 3.545 L 3.438 0.448 C 3.512 0.299 3.438 0.131 3.308 0.038 C 3.159 -0.037 2.992 0.001 2.899 0.131 Z" fill="rgb(0, 0, 0)" height="7.750209501286653px" id="XEy5_M_wF" transform="translate(7.365 2.182)" width="3.470578512630766px"/><path d="M 0.026 1.94 C 0.1 2.07 0.249 2.108 0.379 2.052 L 2.832 0.97 C 2.85 0.97 2.869 0.97 2.887 0.97 L 5.34 2.052 C 5.47 2.108 5.619 2.052 5.693 1.94 C 5.768 1.809 5.731 1.66 5.6 1.585 L 3.222 0.112 C 3.222 0.112 3.036 0 2.869 0 C 2.664 0 2.497 0.112 2.497 0.112 L 0.119 1.585 C 0.007 1.66 -0.03 1.809 0.026 1.94 Z" fill="rgb(0, 0, 0)" height="2.0768899917602535px" id="GVAyPotmc" transform="translate(3.029 9.923)" width="5.731234655014601px"/><path d="M 7.535 2.91 L 4.264 0.187 C 4.264 0.187 4.06 0 3.837 0 C 3.633 0 3.41 0.187 3.41 0.187 L 0.139 2.91 C 0.009 3.003 -0.047 3.171 0.046 3.32 C 0.12 3.469 0.306 3.525 0.455 3.451 L 3.54 1.38 L 3.818 1.212 C 3.837 1.212 3.874 1.212 3.911 1.212 L 4.19 1.38 L 7.275 3.451 C 7.423 3.525 7.591 3.451 7.684 3.32 C 7.758 3.171 7.721 3.003 7.591 2.91 Z" fill="rgb(0, 0, 0)" height="3.483478327665332px" id="UJGiliWlr" transform="translate(2.06 7.592)" width="7.721540951544936px"/><path d="M 0.137 0.026 C 0.007 0.1 -0.031 0.25 0.025 0.38 L 1.103 2.842 C 1.103 2.861 1.103 2.879 1.103 2.898 L 0.025 5.36 C -0.031 5.491 0.025 5.64 0.137 5.715 C 0.267 5.789 0.415 5.752 0.49 5.621 L 1.958 3.234 C 1.958 3.234 2.069 3.047 2.069 2.879 C 2.069 2.674 1.958 2.506 1.958 2.506 L 0.49 0.119 C 0.415 0.007 0.267 -0.03 0.137 0.026 Z" fill="rgb(0, 0, 0)" height="5.752526692867306px" id="DM37PXgJd" transform="translate(0 3.239)" width="2.0691900389284807px"/><path d="M 0.572 7.6 L 3.285 4.318 C 3.285 4.318 3.471 4.112 3.471 3.889 C 3.471 3.683 3.285 3.46 3.285 3.46 L 0.572 0.14 C 0.479 0.009 0.312 -0.047 0.163 0.046 C 0.014 0.121 -0.042 0.307 0.033 0.457 L 2.095 3.553 L 2.263 3.833 C 2.263 3.851 2.263 3.889 2.263 3.926 L 2.095 4.206 L 0.033 7.302 C -0.042 7.451 0.033 7.619 0.163 7.712 C 0.312 7.787 0.479 7.749 0.572 7.619 Z" fill="rgb(0, 0, 0)" height="7.750215230634018px" id="omz1nxiI6" transform="translate(0.922 2.23)" width="3.470588058544221px"/><path d="M 4.007 1.424 C 4.508 1.424 4.897 1.536 5.231 1.759 C 5.565 1.983 5.787 2.29 5.927 2.709 L 7.735 2.709 C 7.513 1.843 7.067 1.173 6.427 0.698 C 5.787 0.223 4.981 0 3.979 0 C 2.977 0 2.504 0.168 1.92 0.531 C 1.308 0.866 0.863 1.368 0.501 2.011 C 0.167 2.653 0 3.379 0 4.217 C 0 5.055 0.167 5.809 0.501 6.423 C 0.835 7.066 1.308 7.568 1.92 7.903 C 2.532 8.267 3.2 8.434 3.979 8.434 C 4.758 8.434 5.76 8.183 6.4 7.708 C 7.04 7.205 7.485 6.563 7.735 5.725 L 5.927 5.725 C 5.62 6.591 4.981 7.01 3.979 7.01 C 2.977 7.01 2.755 6.758 2.337 6.256 C 1.92 5.753 1.725 5.083 1.725 4.189 C 1.725 3.295 1.92 2.625 2.337 2.15 C 2.755 1.648 3.283 1.424 3.979 1.424 Z" fill="rgb(0, 0, 0)" height="8.434076339054002px" id="fGIMtJKmR" transform="translate(15.609 3.128)" width="7.735096310284753px"/><path d="M 6.093 0.503 C 5.481 0.168 4.814 0 4.034 0 C 3.255 0 2.532 0.168 1.92 0.531 C 1.308 0.866 0.835 1.368 0.501 2.011 C 0.167 2.653 0 3.379 0 4.217 C 0 5.055 0.167 5.809 0.529 6.423 C 0.89 7.066 1.363 7.568 1.976 7.903 C 2.588 8.267 3.283 8.434 4.062 8.434 C 4.841 8.434 5.815 8.183 6.455 7.708 C 7.095 7.233 7.54 6.619 7.791 5.865 L 5.982 5.865 C 5.62 6.619 4.98 7.01 4.062 7.01 C 3.144 7.01 2.894 6.814 2.476 6.423 C 2.031 6.032 1.809 5.502 1.753 4.859 L 7.958 4.859 C 7.985 4.608 8.013 4.329 8.013 4.022 C 8.013 3.24 7.846 2.541 7.512 1.927 C 7.179 1.313 6.706 0.838 6.121 0.503 Z M 1.725 3.491 C 1.809 2.849 2.059 2.346 2.476 1.983 C 2.894 1.62 3.395 1.424 3.979 1.424 C 4.563 1.424 5.147 1.62 5.593 1.983 C 6.038 2.346 6.26 2.849 6.26 3.491 L 1.753 3.491 Z" fill="rgb(0, 0, 0)" height="8.434076339054002px" id="qaL5FVZij" transform="translate(24.013 3.128)" width="8.01332295195354px"/><path d="M 5.815 0.391 C 5.314 0.112 4.73 0 4.09 0 C 3.45 0 3.144 0.084 2.727 0.279 C 2.309 0.475 1.948 0.726 1.669 1.061 L 1.669 0.14 L 0 0.14 L 0 8.294 L 1.669 8.294 L 1.669 3.742 C 1.669 3.016 1.864 2.458 2.226 2.067 C 2.587 1.676 3.088 1.48 3.729 1.48 C 4.368 1.48 4.841 1.676 5.231 2.067 C 5.592 2.458 5.787 3.016 5.787 3.742 L 5.787 8.294 L 7.457 8.294 L 7.457 3.491 C 7.457 2.737 7.318 2.122 7.04 1.592 C 6.761 1.061 6.344 0.67 5.843 0.419 Z" fill="rgb(0, 0, 0)" height="8.294435702953454px" id="WDjXqIjZT" transform="translate(33.166 3.128)" width="7.4567073744807075px"/><path d="M 2.643 0 L 0.946 0 L 0.946 2.039 L 0 2.039 L 0 3.407 L 0.946 3.407 L 0.946 7.931 C 0.946 8.741 1.141 9.3 1.558 9.663 C 1.948 10.026 2.532 10.193 3.311 10.193 L 4.647 10.193 L 4.647 8.797 L 3.617 8.797 C 3.283 8.797 3.033 8.741 2.894 8.602 C 2.755 8.462 2.671 8.239 2.671 7.931 L 2.671 3.407 L 4.647 3.407 L 4.647 2.039 L 2.671 2.039 L 2.671 0 Z" fill="rgb(0, 0, 0)" height="10.193494685087567px" id="nZ8KAi6H2" transform="translate(41.458 1.229)" width="4.646524285330045px"/><path d="M 1.085 0 C 0.779 0 0.528 0.112 0.306 0.307 C 0.111 0.503 0 0.782 0 1.089 C 0 1.396 0.111 1.648 0.306 1.871 C 0.501 2.095 0.779 2.178 1.085 2.178 C 1.391 2.178 1.642 2.067 1.836 1.871 C 2.031 1.676 2.142 1.396 2.142 1.089 C 2.142 0.782 2.031 0.531 1.836 0.307 C 1.642 0.112 1.391 0 1.085 0 Z" fill="rgb(0, 0, 0)" height="2.1783368721996954px" id="xofK7bnqV" transform="translate(47.384 0)" width="2.1424521645366994px"/><path d="M 1.669 0 L 0 0 L 0 8.155 L 1.669 8.155 Z" fill="rgb(0, 0, 0)" height="8.154788300335934px" id="owXtEW3wx" transform="translate(47.607 3.267)" width="1.6694896185170123px"/><path d="M 1.085 0 C 0.779 0 0.529 0.112 0.306 0.307 C 0.111 0.503 0 0.782 0 1.089 C 0 1.396 0.111 1.648 0.306 1.871 C 0.501 2.067 0.779 2.178 1.085 2.178 C 1.391 2.178 1.642 2.067 1.836 1.871 C 2.031 1.676 2.142 1.396 2.142 1.089 C 2.142 0.782 2.031 0.531 1.836 0.307 C 1.642 0.112 1.391 0 1.085 0 Z" fill="rgb(0, 0, 0)" height="2.1783368721996954px" id="qYXTLcef6" transform="translate(55.842 0)" width="2.1424521645367136px"/><path d="M 4.007 7.01 C 3.311 7.01 2.783 6.758 2.365 6.256 C 1.948 5.753 1.753 5.083 1.753 4.189 C 1.753 3.295 1.948 2.625 2.365 2.15 C 2.783 1.648 3.311 1.424 4.007 1.424 C 4.702 1.424 4.897 1.536 5.231 1.759 C 5.565 1.983 5.788 2.29 5.926 2.709 L 7.735 2.709 C 7.513 1.843 7.067 1.173 6.427 0.698 C 5.788 0.223 4.981 0 3.979 0 C 2.977 0 2.504 0.168 1.92 0.531 C 1.308 0.866 0.862 1.368 0.501 2.011 C 0.167 2.653 0 3.379 0 4.217 C 0 5.055 0.167 5.809 0.501 6.423 C 0.835 7.066 1.308 7.568 1.92 7.903 C 2.532 8.267 3.2 8.434 3.979 8.434 C 4.758 8.434 5.76 8.183 6.4 7.708 C 7.04 7.205 7.485 6.563 7.735 5.725 L 5.926 5.725 C 5.621 6.591 4.981 7.01 3.979 7.01 Z" fill="rgb(0, 0, 0)" height="8.434076339054002px" id="YVPoMPmqZ" transform="translate(59.265 3.128)" width="7.735226155870485px"/><path d="M 6.872 3.268 L 2.643 3.268 L 2.643 2.681 C 2.643 2.206 2.754 1.871 2.949 1.676 C 3.144 1.508 3.478 1.396 3.923 1.396 L 3.923 0 C 2.921 0 2.17 0.223 1.697 0.642 C 1.196 1.061 0.946 1.759 0.946 2.681 L 0.946 3.268 L 0 3.268 L 0 4.636 L 0.946 4.636 L 0.946 11.422 L 2.643 11.422 L 2.643 4.636 L 5.203 4.636 L 5.203 11.422 L 6.872 11.422 Z" fill="rgb(0, 0, 0)" height="11.422308710362525px" id="mR0Sii5R7" transform="translate(50.863 0)" width="6.872402238697973px"/></g></svg>)
" width="11.757210121961878px"><path d="M 5.706 0.137 C 5.631 0.007 5.483 -0.031 5.353 0.025 L 2.9 1.107 C 2.881 1.107 2.862 1.107 2.844 1.107 L 0.391 0.025 C 0.261 -0.031 0.112 0.025 0.038 0.137 C -0.036 0.268 0.001 0.417 0.131 0.491 L 2.509 1.965 C 2.509 1.965 2.695 2.077 2.862 2.077 C 3.067 2.077 3.234 1.965 3.234 1.965 L 5.613 0.491 C 5.724 0.417 5.761 0.268 5.706 0.137 Z" fill="rgb(255, 255, 255)" height="2.0768733060957265px" id="JOqgQgeXH" transform="translate(2.998 0)" width="5.731236321640178px"/><path d="M 0.187 0.574 L 3.457 3.297 C 3.457 3.297 3.662 3.483 3.885 3.483 C 4.089 3.483 4.312 3.297 4.312 3.297 L 7.582 0.574 C 7.713 0.481 7.768 0.313 7.675 0.163 C 7.601 0.014 7.415 -0.042 7.267 0.033 L 4.182 2.103 L 3.903 2.271 C 3.885 2.271 3.847 2.271 3.81 2.271 L 3.531 2.103 L 0.447 0.033 C 0.298 -0.042 0.131 0.033 0.038 0.163 C -0.036 0.313 0.001 0.481 0.131 0.574 Z" fill="rgb(255, 255, 255)" height="3.483465570588767px" id="Zd5XdemVt" transform="translate(1.975 0.925)" width="7.721539723261137px"/><path d="M 1.933 5.727 C 2.063 5.652 2.1 5.503 2.044 5.372 L 0.966 2.91 C 0.966 2.892 0.966 2.873 0.966 2.854 L 2.044 0.392 C 2.1 0.262 2.044 0.113 1.933 0.038 C 1.803 -0.037 1.654 0.001 1.58 0.131 L 0.112 2.519 C 0.112 2.519 0 2.705 0 2.873 C 0 3.078 0.112 3.246 0.112 3.246 L 1.58 5.634 C 1.654 5.745 1.803 5.783 1.933 5.727 Z" fill="rgb(255, 255, 255)" height="5.752520201428616px" id="wm4QOyIBO" transform="translate(9.688 3.009)" width="2.069203720899866px"/><path d="M 2.899 0.187 L 0.186 3.47 C 0.186 3.47 0 3.675 0 3.899 C 0 4.104 0.186 4.328 0.186 4.328 L 2.899 7.611 C 2.992 7.741 3.159 7.797 3.308 7.704 C 3.456 7.629 3.512 7.443 3.438 7.294 L 1.375 4.197 L 1.208 3.918 C 1.208 3.899 1.208 3.862 1.208 3.824 L 1.375 3.545 L 3.438 0.448 C 3.512 0.299 3.438 0.131 3.308 0.038 C 3.159 -0.037 2.992 0.001 2.899 0.131 Z" fill="rgb(255, 255, 255)" height="7.750209542168115px" id="Tb0_95onW" transform="translate(7.365 1.983)" width="3.470578512630766px"/><path d="M 0.026 1.94 C 0.1 2.07 0.249 2.108 0.379 2.052 L 2.832 0.97 C 2.85 0.97 2.869 0.97 2.887 0.97 L 5.34 2.052 C 5.47 2.108 5.619 2.052 5.693 1.94 C 5.768 1.809 5.731 1.66 5.6 1.585 L 3.222 0.112 C 3.222 0.112 3.036 0 2.869 0 C 2.664 0 2.497 0.112 2.497 0.112 L 0.119 1.585 C 0.007 1.66 -0.03 1.809 0.026 1.94 Z" fill="rgb(255, 255, 255)" height="2.07689008196461px" id="mLkmMllwc" transform="translate(3.029 9.724)" width="5.731234655014603px"/><path d="M 7.535 2.91 L 4.264 0.187 C 4.264 0.187 4.06 0 3.837 0 C 3.633 0 3.41 0.187 3.41 0.187 L 0.139 2.91 C 0.009 3.003 -0.047 3.171 0.046 3.32 C 0.12 3.469 0.306 3.525 0.455 3.451 L 3.54 1.38 L 3.818 1.212 C 3.837 1.212 3.874 1.212 3.911 1.212 L 4.19 1.38 L 7.275 3.451 C 7.423 3.525 7.591 3.451 7.684 3.32 C 7.758 3.171 7.721 3.003 7.591 2.91 Z" fill="rgb(255, 255, 255)" height="3.483478327665331px" id="r0d9h4JTL" transform="translate(2.06 7.392)" width="7.7215409515449345px"/><path d="M 0.137 0.026 C 0.007 0.1 -0.031 0.25 0.025 0.38 L 1.103 2.842 C 1.103 2.861 1.103 2.879 1.103 2.898 L 0.025 5.36 C -0.031 5.491 0.025 5.64 0.137 5.715 C 0.267 5.789 0.415 5.752 0.49 5.621 L 1.958 3.234 C 1.958 3.234 2.069 3.047 2.069 2.879 C 2.069 2.674 1.958 2.506 1.958 2.506 L 0.49 0.119 C 0.415 0.007 0.267 -0.03 0.137 0.026 Z" fill="rgb(255, 255, 255)" height="5.752526692867306px" id="yi3WcGLKq" transform="translate(0 3.04)" width="2.0691900389284807px"/><path d="M 0.572 7.6 L 3.285 4.318 C 3.285 4.318 3.471 4.112 3.471 3.889 C 3.471 3.683 3.285 3.46 3.285 3.46 L 0.572 0.14 C 0.479 0.009 0.312 -0.047 0.163 0.046 C 0.014 0.121 -0.042 0.307 0.033 0.457 L 2.095 3.553 L 2.263 3.833 C 2.263 3.851 2.263 3.889 2.263 3.926 L 2.095 4.206 L 0.033 7.302 C -0.042 7.451 0.033 7.619 0.163 7.712 C 0.312 7.787 0.479 7.749 0.572 7.619 Z" fill="rgb(255, 255, 255)" height="7.750215283552243px" id="p6XslZnAU" transform="translate(0.922 2.031)" width="3.4705880585442213px"/></g><path d="M 4.007 1.424 C 4.508 1.424 4.897 1.536 5.231 1.759 C 5.565 1.983 5.787 2.29 5.927 2.709 L 7.735 2.709 C 7.513 1.843 7.067 1.173 6.427 0.698 C 5.787 0.223 4.981 0 3.979 0 C 2.977 0 2.504 0.168 1.92 0.531 C 1.308 0.866 0.863 1.368 0.501 2.011 C 0.167 2.653 0 3.379 0 4.217 C 0 5.055 0.167 5.809 0.501 6.423 C 0.835 7.066 1.308 7.568 1.92 7.903 C 2.532 8.267 3.2 8.434 3.979 8.434 C 4.758 8.434 5.76 8.183 6.4 7.708 C 7.04 7.205 7.485 6.563 7.735 5.725 L 5.927 5.725 C 5.62 6.591 4.981 7.01 3.979 7.01 C 2.977 7.01 2.755 6.758 2.337 6.256 C 1.92 5.753 1.725 5.083 1.725 4.189 C 1.725 3.295 1.92 2.625 2.337 2.15 C 2.755 1.648 3.283 1.424 3.979 1.424 Z" fill="rgb(255, 255, 255)" height="8.434076339054002px" id="d2DNCsqwq" transform="translate(15.609 3.128)" width="7.735096310284753px"/><path d="M 6.093 0.503 C 5.481 0.168 4.814 0 4.034 0 C 3.255 0 2.532 0.168 1.92 0.531 C 1.308 0.866 0.835 1.368 0.501 2.011 C 0.167 2.653 0 3.379 0 4.217 C 0 5.055 0.167 5.809 0.529 6.423 C 0.89 7.066 1.363 7.568 1.976 7.903 C 2.588 8.267 3.283 8.434 4.062 8.434 C 4.841 8.434 5.815 8.183 6.455 7.708 C 7.095 7.233 7.54 6.619 7.791 5.865 L 5.982 5.865 C 5.62 6.619 4.98 7.01 4.062 7.01 C 3.144 7.01 2.894 6.814 2.476 6.423 C 2.031 6.032 1.809 5.502 1.753 4.859 L 7.958 4.859 C 7.985 4.608 8.013 4.329 8.013 4.022 C 8.013 3.24 7.846 2.541 7.512 1.927 C 7.179 1.313 6.706 0.838 6.121 0.503 Z M 1.725 3.491 C 1.809 2.849 2.059 2.346 2.476 1.983 C 2.894 1.62 3.395 1.424 3.979 1.424 C 4.563 1.424 5.147 1.62 5.593 1.983 C 6.038 2.346 6.26 2.849 6.26 3.491 L 1.753 3.491 Z" fill="rgb(255, 255, 255)" height="8.434076339054002px" id="NZQSgmK3B" transform="translate(24.013 3.128)" width="8.01332295195354px"/><path d="M 5.815 0.391 C 5.314 0.112 4.73 0 4.09 0 C 3.45 0 3.144 0.084 2.727 0.279 C 2.309 0.475 1.948 0.726 1.669 1.061 L 1.669 0.14 L 0 0.14 L 0 8.294 L 1.669 8.294 L 1.669 3.742 C 1.669 3.016 1.864 2.458 2.226 2.067 C 2.587 1.676 3.088 1.48 3.729 1.48 C 4.368 1.48 4.841 1.676 5.231 2.067 C 5.592 2.458 5.787 3.016 5.787 3.742 L 5.787 8.294 L 7.457 8.294 L 7.457 3.491 C 7.457 2.737 7.318 2.122 7.04 1.592 C 6.761 1.061 6.344 0.67 5.843 0.419 Z" fill="rgb(255, 255, 255)" height="8.294435702953454px" id="y4C5qOSA0" transform="translate(33.166 3.128)" width="7.4567073744807075px"/><path d="M 2.643 0 L 0.946 0 L 0.946 2.039 L 0 2.039 L 0 3.407 L 0.946 3.407 L 0.946 7.931 C 0.946 8.741 1.141 9.3 1.558 9.663 C 1.948 10.026 2.532 10.193 3.311 10.193 L 4.647 10.193 L 4.647 8.797 L 3.617 8.797 C 3.283 8.797 3.033 8.741 2.894 8.602 C 2.755 8.462 2.671 8.239 2.671 7.931 L 2.671 3.407 L 4.647 3.407 L 4.647 2.039 L 2.671 2.039 L 2.671 0 Z" fill="rgb(255, 255, 255)" height="10.193494685087567px" id="HConpA1k2" transform="translate(41.458 1.229)" width="4.646524285330045px"/><path d="M 1.085 0 C 0.779 0 0.528 0.112 0.306 0.307 C 0.111 0.503 0 0.782 0 1.089 C 0 1.396 0.111 1.648 0.306 1.871 C 0.501 2.095 0.779 2.178 1.085 2.178 C 1.391 2.178 1.642 2.067 1.836 1.871 C 2.031 1.676 2.142 1.396 2.142 1.089 C 2.142 0.782 2.031 0.531 1.836 0.307 C 1.642 0.112 1.391 0 1.085 0 Z" fill="rgb(255, 255, 255)" height="2.1783368721996954px" id="EuoH5GVjb" transform="translate(47.384 0)" width="2.1424521645366994px"/><path d="M 1.669 0 L 0 0 L 0 8.155 L 1.669 8.155 Z" fill="rgb(255, 255, 255)" height="8.154788300335934px" id="zg308Vtf3" transform="translate(47.607 3.267)" width="1.6694896185170123px"/><path d="M 1.085 0 C 0.779 0 0.529 0.112 0.306 0.307 C 0.111 0.503 0 0.782 0 1.089 C 0 1.396 0.111 1.648 0.306 1.871 C 0.501 2.067 0.779 2.178 1.085 2.178 C 1.391 2.178 1.642 2.067 1.836 1.871 C 2.031 1.676 2.142 1.396 2.142 1.089 C 2.142 0.782 2.031 0.531 1.836 0.307 C 1.642 0.112 1.391 0 1.085 0 Z" fill="rgb(255, 255, 255)" height="2.1783368721996954px" id="SaMxhxR35" transform="translate(55.842 0)" width="2.1424521645367136px"/><path d="M 4.007 7.01 C 3.311 7.01 2.783 6.758 2.365 6.256 C 1.948 5.753 1.753 5.083 1.753 4.189 C 1.753 3.295 1.948 2.625 2.365 2.15 C 2.783 1.648 3.311 1.424 4.007 1.424 C 4.702 1.424 4.897 1.536 5.231 1.759 C 5.565 1.983 5.788 2.29 5.926 2.709 L 7.735 2.709 C 7.513 1.843 7.067 1.173 6.427 0.698 C 5.788 0.223 4.981 0 3.979 0 C 2.977 0 2.504 0.168 1.92 0.531 C 1.308 0.866 0.862 1.368 0.501 2.011 C 0.167 2.653 0 3.379 0 4.217 C 0 5.055 0.167 5.809 0.501 6.423 C 0.835 7.066 1.308 7.568 1.92 7.903 C 2.532 8.267 3.2 8.434 3.979 8.434 C 4.758 8.434 5.76 8.183 6.4 7.708 C 7.04 7.205 7.485 6.563 7.735 5.725 L 5.926 5.725 C 5.621 6.591 4.981 7.01 3.979 7.01 Z" fill="rgb(255, 255, 255)" height="8.434076339054002px" id="HetImuuV4" transform="translate(59.265 3.128)" width="7.735226155870485px"/><path d="M 6.872 3.268 L 2.643 3.268 L 2.643 2.681 C 2.643 2.206 2.754 1.871 2.949 1.676 C 3.144 1.508 3.478 1.396 3.923 1.396 L 3.923 0 C 2.921 0 2.17 0.223 1.697 0.642 C 1.196 1.061 0.946 1.759 0.946 2.681 L 0.946 3.268 L 0 3.268 L 0 4.636 L 0.946 4.636 L 0.946 11.422 L 2.643 11.422 L 2.643 4.636 L 5.203 4.636 L 5.203 11.422 L 6.872 11.422 Z" fill="rgb(255, 255, 255)" height="11.422308710362525px" id="Xc4NeSznw" transform="translate(50.863 0)" width="6.872402238697973px"/></g></svg>)


7 min read time
AI Summary by Centific
Turn this article into insights
with AI-powered summaries
Topics

Prasanna Desikan

Harshit Rajgarhia
Shivali Dalmia
Ananya Mantravadi
Healthcare AI is advancing faster than healthcare industry’s ability to evaluate it. As systems become multimodal and agentic, today’s benchmarks still measure narrow accuracy rather than whether a system can be trusted in real clinical use. Benchmarks are structured evaluation systems built for clinical alignment, safety, and reproducibility.
These ideas were the focus of a tutorial, “Measuring What Matters: Benchmarking Generative, Multimodal, and Agentic AI in Healthcare,” delivered by Centific’s AI Research Team at the IEEE International Conference on Healthcare Informatics (IEEE ICHI 2026) in Minneapolis, Minnesota on June 1-3. The session resonated with practitioners. As one participant, Dr. Ram D. Sriram, Senior Advisor, National Institute of Standards and Technology (NIST), reflected on the discussion: “Very informative panel and tutorial. Kudos to Prasanna Desikan for coordinating these.” (This was his personal feedback, not an endorsement by NIST.)
That kind of engagement reflected a broader recognition in the room: that healthcare AI evaluation needs to change, and that there is a concrete case for what a better approach looks like.
Why evaluation through benchmarks matters
Benchmarks are critical because they provide a structured and repeatable way to measure how a system performs in real-world tasks and provide insights on whether it is ready to move from prototype to production.
Modern healthcare AI systems are built on large foundation models adapted through prompting, fine-tuning, and retrieval (pulling in EHR data, clinical guidelines, and medical literature). Because development is guided so heavily by benchmark performance, benchmarks actively shape how these systems behave and which capabilities model builders choose to optimize for.
The core problem: evaluation hasn’t kept pace
Generative and specialized healthcare models (GPT-4/5-class, Gemini, Claude, plus Med-PaLM, MedGemma, BioClinicalBERT) are being rapidly integrated into clinical workflows, but evaluations have not kept pace with model capability.
Evaluation methods fall short for two reasons:
First, healthcare AI is now multimodal, spanning clinical notes, imaging, audio, and sensor data, and embedded in real workflows such as documentation, triage, and care coordination. Performance therefore has to be judged in context, not in isolation.
Second, there’s been a shift from models to systems. Earlier work evaluated single-task models (e.g., BioBERT/ClinicalBERT for text extraction), whereas modern systems combine retrieval, reasoning, and generation into end-to-end workflows. Their behavior depends on interactions between components, not just individual model accuracy.
Centific’s recommendation: design benchmarks that measure what matters
Most healthcare AI evaluation today asks a narrow question: “Did the model produce the right answer?” The real question is, “Can this system be trusted to support a clinical decision?”
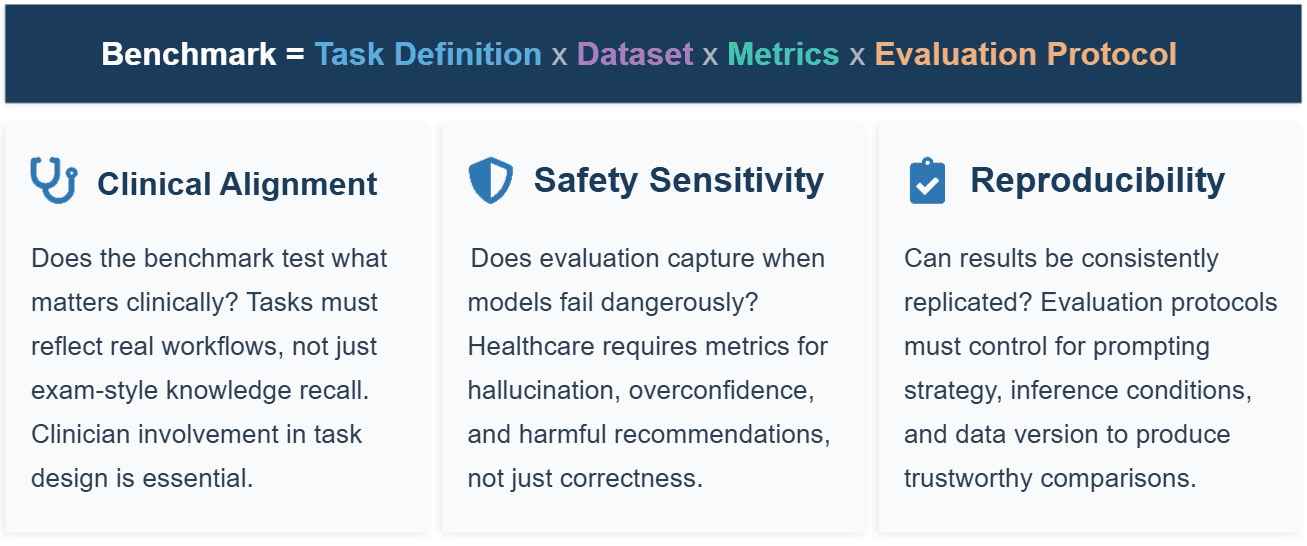
We recommend that healthcare AI benchmarks be treated not as datasets but as structured evaluation systems designed for reproducible, comparable measurement of model capability. We also recommend that every benchmark be specified across four elements:
Task definition (the problem being solved, such as diagnosis or triage)
Dataset (curated inputs, labels, and splits)
Metrics (how performance is measured, from accuracy to calibration)
Evaluation protocol (how evaluation is run end-to-end, including prompting, rubric-based scoring, and aggregation). For healthcare in particular, benchmarks should demonstrate clinical alignment, safety sensitivity, and reproducibility.
Our recommended approach to benchmarking healthcare AI rests on five connected ideas:
Build evaluation as a system, not just an accuracy score
A benchmark is only as good as what it’s built on. Rather than a single score, a strong benchmark is a structured evaluation system. That starts with task design, defining the real clinical task with the right inputs, context, and success conditions, rather than a simplified proxy. It rests on a repeatable process, treating benchmark creation as a disciplined lifecycle that scopes the task, sources representative data, defines evaluation metrics, and then runs, validates, documents, and iterates, so that results are reproducible rather than one-off. And it relies on multi-metric measurements because no single number captures clinical fitness. Every task is scored across complementary dimensions such as accuracy, calibration, safety, and reliability, rather than reduced to a lone leaderboard figure.
Match the rigor of evaluation to the risk of the task
Not all AI tasks carry the same consequences, so they shouldn’t be held to the same evaluation bar. We propose a maturity ladder with three tiers:
Document and communicate (lowest risk): tasks like summarizing or drafting clinical notes. Here, the stakes are clarity and faithfulness, so the right measures are text-fidelity scores (e.g., semantic similarity) paired with a hallucination/fabrication rate, evaluated on de-identified notes.
Detect and interpret (moderate risk): tasks like flagging findings or interpreting multimodal patient data. Because a wrong call has clinical weight, evaluation must include discrimination and calibration measures (e.g., AUROC, expected calibration error) and sensitivity, which needs to be tested across the data clinicians use: records, imaging, and audio together.
Act and coordinate (highest risk): tasks where the system takes or orchestrates actions, such as navigating a record system or coordinating steps of care. Here, outcome-level measures matter most. Did the system complete the task correctly and follow the right steps? This needs to be validated in a simulated live clinical environment using clinician-authored scenarios.
This tiering tells builders, reviewers, and buyers exactly how much evidence is required before a given capability is trusted in practice.
Evaluate agents on the whole job, not a single answer
When AI moves from answering questions to doing tasks, single-turn accuracy stops being meaningful. Centific performed a test with agentic AI that illustrates this point: starting from an action-oriented benchmark, we ran a broad set of leading models through realistic multi-step clinical tasks and found that conventional scoring badly overstated competence — a “do-nothing” baseline scored deceptively well, and even the strongest models cleared only a small fraction of the hardest tasks. The lesson is that agentic systems must be measured on the full sequence of actions and the outcome, in an environment that responds dynamically, reacting to each action and surfacing mistakes.
Treat multimodal, longitudinal care as the default because it is
Real clinical reasoning draws on many signals at once across notes, images, labs, audio, and across a patient’s history over time, yet most benchmarks still test one modality in isolation. Research attention to multimodal evaluation has grown sharply in recent years, but the tooling hasn’t caught up. We recommend benchmarks that combine modalities and unfold over time, reflecting how care is actually delivered.
For systems that learn or plan over time, score the trajectory, not the step
Many clinical workflows involve delayed consequences and information that isn’t fully visible the moment the decision is made; however, the value of an action only becomes clear later. Evaluation should mirror this by judging the entire path a system takes toward an outcome, accounting for delayed payoff and hidden state, rather than grading each step in isolation.
What’s next: a shared effort to evaluate AI as deployed systems
Healthcare AI evaluation has to move away from static, single-task scoring and toward governed, longitudinal, action-verifiable environments. These are settings that judge a system on what it actually does over time, under real-world conditions, rather than on isolated answers to isolated questions.
No single organization can build this evaluation infrastructure alone. Better benchmarks depend on better data and on shared evaluation infrastructure, which makes this a distributed effort across the field, from researchers, clinicians, health systems, to industry players, each contributing a piece. Progress will come from collaboration, not from any one team's leaderboard.
Centific can serve as a data and benchmarking partner. Centific can supply three elements needed to evaluate healthcare AI the way it is deployed:
Realistic, multi-signal datasets tied to real outcomes
A consistent set of metrics
Clear rubrics that define how performance is scored
Each is built to meet governance and compliance requirements.
If you are building, validating, or governing healthcare AI and want to help raise the bar for how it is measured, we would welcome the conversation.
Meanwhile, here is a link to our tutorial paper for more context.
Learn more about Centific’s healthcare AI capabilities.
Are your ready to get
modular
AI solutions delivered?
Connect data, models, and people — in one enterprise-ready platform.
Latest Insights



Connect with Centific
Updates from the frontier of AI data.
Receive updates on platform improvements, new workflows, evaluation capabilities, data quality enhancements, and best practices for enterprise AI teams.